
#WeCount is a reporting effort that captures monthly shifts in the volume of abortions provided within the formal US healthcare system, nationally and by state, following the Dobbs v Jackson Women’s Health Organization Supreme Court decision to overturn Roe v Wade. This report includes data from April 2022 to December 2025.
#WeCount data explorer
| State | Month | Total abortions | In-person | Total telehealth | Virtual-only telehealth | Brick-and-mortar telehealth |
|---|
Key findings
- Across the US, 1.13 million abortions were provided in the formal healthcare system in 2025.
- The number of abortions remains higher than before Dobbs.
- The monthly average number of abortions was slightly higher in 2025 than it was in 2024.
- Nationally, the majority of abortions occurred in person; the number of in-person abortions decreased slightly between 2024 and 2025.
- The number of abortions provided via telehealth has increased; across 2025, over 300,000 abortions were provided via telehealth.
- By December 2025, 29% of US abortions were provided via telehealth.
- Shield laws continue to facilitate abortion access, with nearly 15,000 abortions per month provided under shield laws by December 2025.
Download the data
The following resources are available for download:
- Report data tables [.xlsx]
- Summary slides with national and 51 state-level findings [.pptx]
- Report narrative [.pdf]
- Press release [.pdf]
Contact WeCount@SocietyFP.org if you would like to explore the data via additional formats.
Please use the citation below to cite this #WeCount report.
Society of Family Planning. #WeCount Report April 2022 through December 2025. 10 Jun. 2026, https://societyfp.org/research/wecount/wecount-december-2025-data/, https://doi.org/10.46621/793758dfrane.
National findings
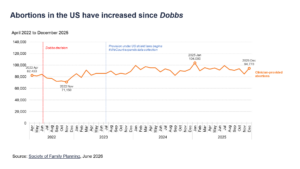
Abortions in the US have increased since Dobbs
The monthly number of abortions increased gradually over time in the US since 2022. The monthly total peaked in January 2025, reaching 104,000 abortions in a single month.
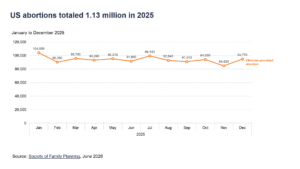
US abortions totaled 1.13 million in 2025
Across 2025, a total of 1,126,760 abortions were provided in the US healthcare system.
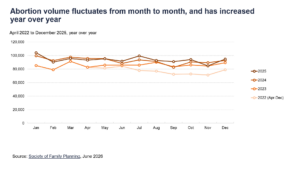
Abortion volume fluctuates from month to month, and has increased year over year
In addition to some monthly fluctuation, abortion volume has increased year over year. For most months, 2025 abortion counts were similar to 2024.
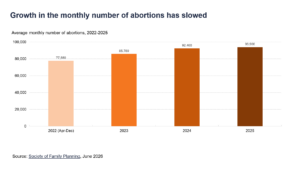
Growth in the monthly number of abortions has slowed
The monthly average number of abortions climbed from 77,560 in 2022, to 85,780 in 2023, to 92,400 in 2024, to 93,900 in 2025. Note that the 2022 monthly average reflects a partial year of data.
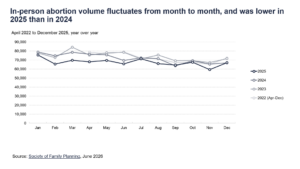
In-person abortion volume fluctuates from month to month, and was lower in 2025 than in 2024
In addition to some monthly fluctuation, in-person abortion volume has decreased slightly, with monthly numbers in 2025 lower than in 2024. Monthly abortion volume was typically higher in the first half of each year.
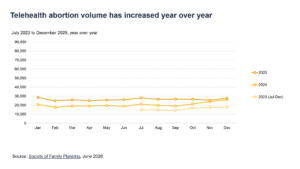
Telehealth abortion volume has increased year over year
Telehealth abortion volume does not fluctuate substantially from month to month and has increased year over year.
Telehealth findings
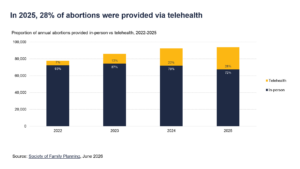
In 2025, 28% of abortions were provided via telehealth
The proportion of abortions provided via telehealth has increased each year between 2022 and 2025.
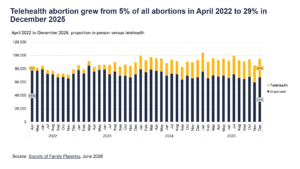
Telehealth abortion grew from 5% of all abortions in April 2022 to 29% in December 2025
The proportion of abortions provided via telehealth increased from 5% in April 2022 to 29% in December 2025.
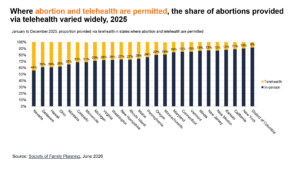
Where abortion and telehealth are permitted, the share of abortions provided via telehealth varied widely, 2025
Across the US, in states that permit abortion and telehealth provision of abortion, there was substantial variation in the proportion of abortions provided via telehealth, ranging from 8% to 44%. In several larger population states (eg, New York, California, Illinois, and New Jersey), telehealth represents a smaller share of abortions, at 10-13% of all abortions.
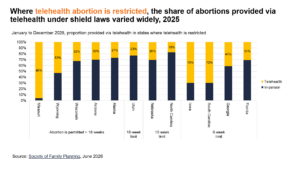
Where telehealth abortion is restricted, the share of abortions provided via telehealth under shield laws varied widely, 2025
In states without a total abortion ban but where telehealth is restricted, including states with 6, 12, and 18-week bans, the proportion of abortions provided by telehealth varies widely.
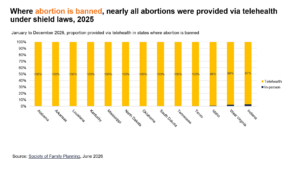
Where abortion is banned, nearly all abortions were provided via telehealth under shield laws, 2025
In states with total abortion bans, telehealth abortions provided under shield laws make up nearly all abortions occurring within those states. Residents may travel to other states to obtain care. Abortions provided in person under exceptions are represented in dark blue, making up 3% of abortions in Indiana, 2% of abortions in West Virginia, and 1% of abortions in Idaho. In North Dakota, no abortion facilities were providing in-person care from January to November 2025, when the state implemented a total ban.
Over half of telehealth abortions are now provided under shield laws
The number and proportion of telehealth abortions provided under shield laws has increased over time. As of December 2025, more than half (54%) of telehealth abortions are provided under shield laws.
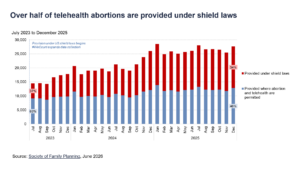
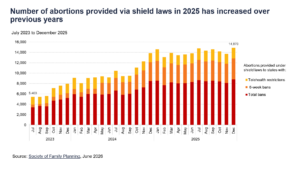
Number of abortions provided via shield laws in 2025 has increased over previous years
By December 2025, abortions provided under shield laws totaled 14,870 per month. Shield laws provide protections for clinicians to mail medication abortion pills to people in states with telehealth restrictions, 6-week bans, and total abortion bans. The number of abortions provided under shield laws into states with these restrictions has increased since clinicians began to offer abortion under shield laws in July 2023, with notable increases in provision to states after enactment of 6-week bans and total abortion bans. Some of the increase in states with 6-week bans is due to changes in state-level restrictions, such as states that transitioned from telehealth restrictions to 6-week bans during this period and thus switched categories.
Background
#WeCount is a national effort that reports monthly numbers of abortions in the US, nationally and by state, beginning in April 2022. #WeCount data include abortions within the formal US healthcare system, defined as medication or procedural abortions provided by a licensed US clinician operating within their licensed scope of practice.
#WeCount data do not reflect self-managed abortions, defined as ending a pregnancy without the involvement of a licensed clinician operating within their licensed scope of practice, such as medications provided by community networks, clinicians providing care outside their licensed scope of practice, or websites that sell medications outside of the formal US healthcare system.
These data reflect the status of abortion provision within the formal US healthcare system and can help healthcare systems, public health practitioners, and policymakers make evidence-informed decisions. Monthly state totals were rounded to the nearest 10.
Terminology
State of occurrence
- In-person care: The state where the healthcare facility providing the abortion is located.
- Telehealth care: The state to which abortion medications are mailed.
Delivery settings
- Brick and mortar clinic: A physical clinic where a patient can go to receive care.
- Virtual-only clinic: An online-only provider.
Delivery methods
- Brick-and-mortar telehealth: Telehealth abortions offered by a brick-and-mortar clinic.
- In-person care: Abortions in which a clinician meets with the patient face-to-face; can be procedural or medication abortions.
- Telehealth abortion: Medication abortion offered by a clinician through remote consultation with the patient, resulting in remote dispensing of medications by mail.
- Self-managed abortions: Note that #WeCount does not include self-managed abortions, defined as abortions using medications, herbs, or something else, or obtaining pills from friends or online without clinician assistance.
Types of care
- Medication abortion: Abortion performed with medications, including mifepristone, misoprostol, or misoprostol alone.
- Procedural abortion: Abortion performed with instrumentation, including uterine aspiration (manual or electric), dilation and curettage, dilation and evacuation, or dilation and extraction.
Legal context
- Shield laws: Shield laws provide protections for clinicians to mail medication abortion pills to people in states with telehealth restrictions, 6-week bans, and total abortion bans.
Methods
Provider database
In early 2022, #WeCount developed a database of all known US abortion facilities, including clinics, private medical offices, hospitals, and virtual clinic providers. We used the Abortion Facility Database from Advancing New Standards in Reproductive Health (ANSIRH) at University of California, San Francisco to establish a clinic database, and continue to update our list throughout the study period using annual updates to ANSIRH’s abortion facility database, abortion directories (AbortionFinder.org and INeedanA.com) and word-of-mouth referrals to unlisted abortion-providing facilities and clinicians.
Data collection
#WeCount collects monthly abortion volume data from participating facilities and offers remuneration for each monthly submission.
Missing data and imputation
The data in this report includes the monthly counts reported by providers for April 2022 through December 2025. From April 2022 to December 2024, 11% of abortions were imputed. From January to December 2025, 22% of abortions were imputed. The magnitude of imputation in each state is noted with symbols in the data tables.
In-person providers:
- Partial reporting: For providers missing some months of data, we imputed values for missing months based on the average percent month-to-month change in in-person abortion volume in the state.
- Non-reporting: For providers that never reported, we estimated all months of data using contextual information, including news articles, contacts known to the non-reporting clinics, knowledge of the abortion volumes by state, and state-level medians from reporting facilities. To compute medians, we categorized reporters to #WeCount into five types of facilities: 1) small abortion clinics, 2) large abortion clinics, 3) primary care clinics, 4) low volume hospitals, and 5) high volume hospitals. Where available, we also used publicly available state administrative data to supplement our estimates.
Virtual clinics:
- Partial reporting: For virtual clinics missing some months of data, we imputed values for missing months based on the average percent month-to-month change in virtual clinic abortion volume in the state.
- Non-reporting: We developed separate imputations for virtual clinics that did not submit data to us, using the median number of abortions that were provided by other virtual clinics in the state.
State policy environment
We reported the number of abortions by state and by restrictiveness level using several categories. These categories were based on the abortion policy in each state on the 15th of each month as reported by the New York Times. For a legal analysis of restrictions that explicitly ban telehealth or implicitly preclude telehealth abortion, we rely on the RHITES map.
- Total abortion bans: States that restrict abortion at all gestations, with or without exceptions.
- 6-week abortion bans: States that restrict abortion after detection of embryonic cardiac activity, referred to as a “6-week bans” because detection of such activity usually occurs around that point.
- 12- to 18-week abortion bans: States that restrict abortion beginning between 12 and 18 weeks of pregnancy.
- Permitted: States where abortion is permitted beyond the gestational categories above. Within permitted states, we disaggregated between states where telehealth abortion is permitted and states where telehealth abortion is restricted.
#WeCount was deemed exempt by Advarra IRB. This research was sponsored by the Society of Family Planning.
Limitations
#WeCount data does not reflect interstate travel for abortion care. As a result, observed changes in abortion volume in some states may reflect changes in interstate travel for abortion.
More abortions in #WeCount were imputed in 2025 than in previous years. This increase in missing data reduces the precision of our estimates.
Counts are likely an underrepresentation of all abortions in the US. #WeCount has a comprehensive count of abortions provided in the formal US healthcare system, with more than 85% of all abortions reported. However, abortions provided by individual hospitals and private practice clinicians may be underreported. These counts also do not include abortions that take place in the US outside of the formal healthcare system.
#WeCount reports abortion service type by distinguishing telehealth from in-person abortion care. #WeCount does not report medication abortions separately from procedural abortions. Thus, the in-person abortion counts include both medication and procedural abortions that were provided in clinics, while all telehealth abortions are medication abortions.
Telehealth data represent the number of medications prescribed, dispensed or mailed by providers. #WeCount cannot estimate the proportion of people who did not take the medications sent to them, and therefore telehealth estimates may overestimate the number of abortions completed.
Use of shield laws to provide abortion via telehealth into states with total or 6-week abortion bans or with telehealth abortion restrictions started in July 2023, and #WeCount began to count abortions provided under shield laws at that time. Because of this transition in abortion provision, #WeCount does not have a comparator for previous months.
#WeCount cannot estimate unmet needs for abortion. Research has yet to accurately capture the underlying need for abortion.
Contributors
#WeCount is made possible by the many abortion providers who generously reported their data in support of this effort, as well as many members of the Society of Family Planning community. This report was prepared by the #WeCount Co-Chairs and Society of Family Planning staff.
#WeCount Co-Chairs
- Alison Norris, MD, PhD; Ohio State University
- Ushma Upadhyay, PhD, MPH; University of California, San Francisco
#WeCount Society of Family Planning staff
- Leah Koenig, PhD, MSPH; #WeCount Director
- Jenny O’Donnell, ScD, MS; Vice President of Research and Evaluation
- Claire Yuan, MPP; #WeCount Data Manager
Contact us
For media inquiries, please contact SFP@ConwayStrategic.com.
For questions about #WeCount and information on how to enroll your practice, please contact WeCount@SocietyFP.org.