
Author: Society of Family Planning
Published: June 23, 2025
#WeCount is a time-limited reporting effort that aims to capture national shifts in abortion volume, by state and month, following the Dobbs v. Jackson Women’s Health Organization Supreme Court decision to overturn Roe v. Wade. This report includes data from April 2022 to December 2024.
For media inquiries, please contact SFP@ConwayStrategic.com.
For questions about #WeCount and information on how to enroll your practice, please contact WeCount@SocietyFP.org.
Please use the citation below to cite this #WeCount report.
Society of Family Planning. #WeCount Report April 2022 through December 2024. 23 Jun. 2025, https://societyfp.org/wecount-report-9-december-2024-data/, https://doi.org/10.46621/725961gzsnai.
Explore the data
The following resources are available for download:
- Report data tables [.xlsx]
- Summary slides with national and 51 state-level findings [.pptx]
- Report narrative [.pdf]
- Press release [.pdf]
Please contact WeCount@SocietyFP.org if there is a way the Society can support your exploration and use of these findings.
Key findings
- Abortion volume is higher in 2024 than it was in 2023 or 2022.
- The majority of abortions occurred in-person.
- The number of abortions delivered via telehealth has continued to increase since April 2022, when #WeCount became the first national study to track telehealth.
- By the end of 2024, 1 in 4 abortions was provided via telehealth.
- Shield laws continue to facilitate the receipt of medication abortion, with an average of 12,330 abortions per month provided under shield laws by the end of 2024.
- Drivers of these trends are unclear, especially in the context of multiple changes in the service delivery environment; new evidence that helps contextualize these findings continues to emerge.
National findings
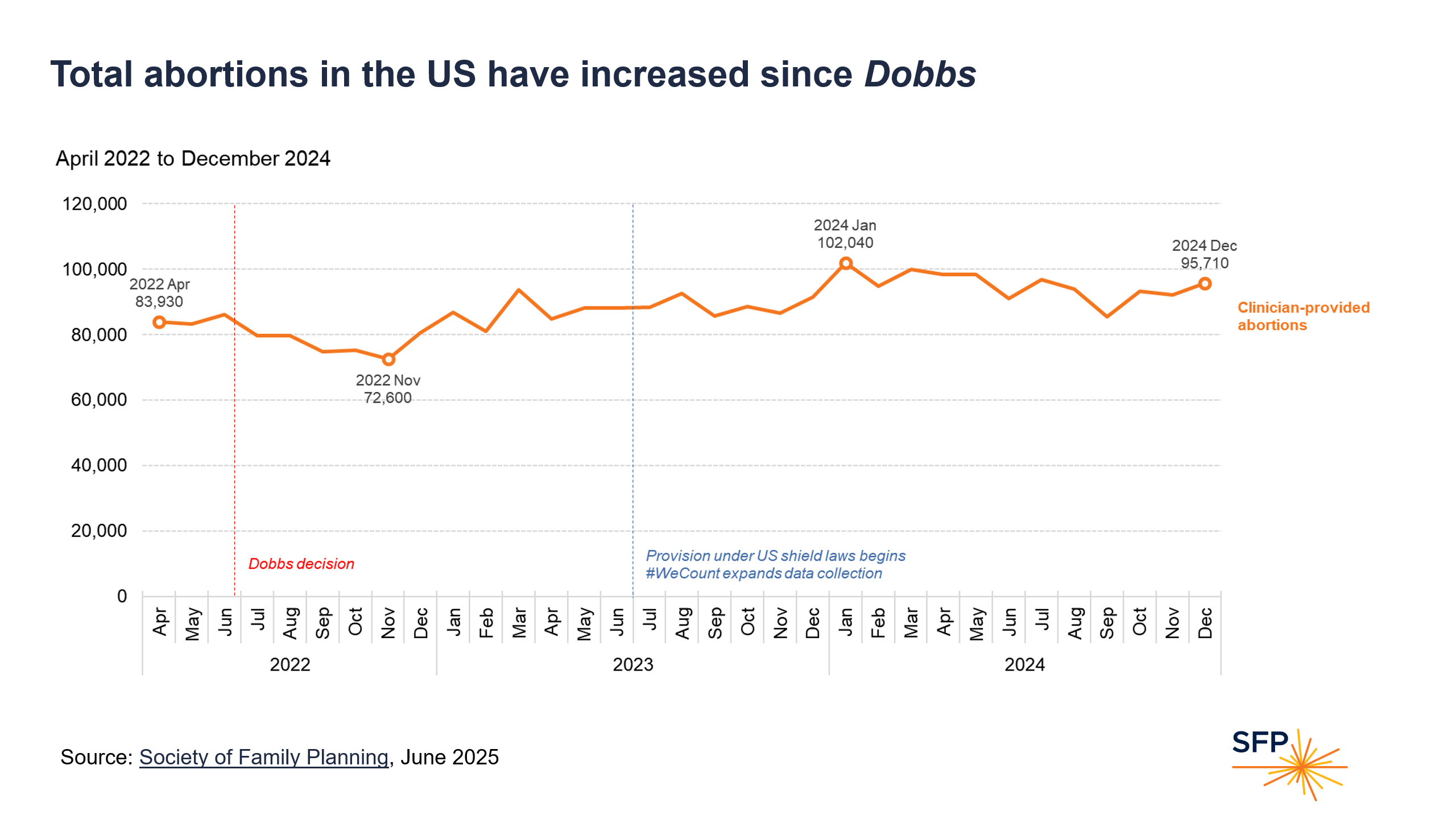
Total abortions in the US have increased since Dobbs
The monthly number of abortions increased gradually over time in the US since 2022.
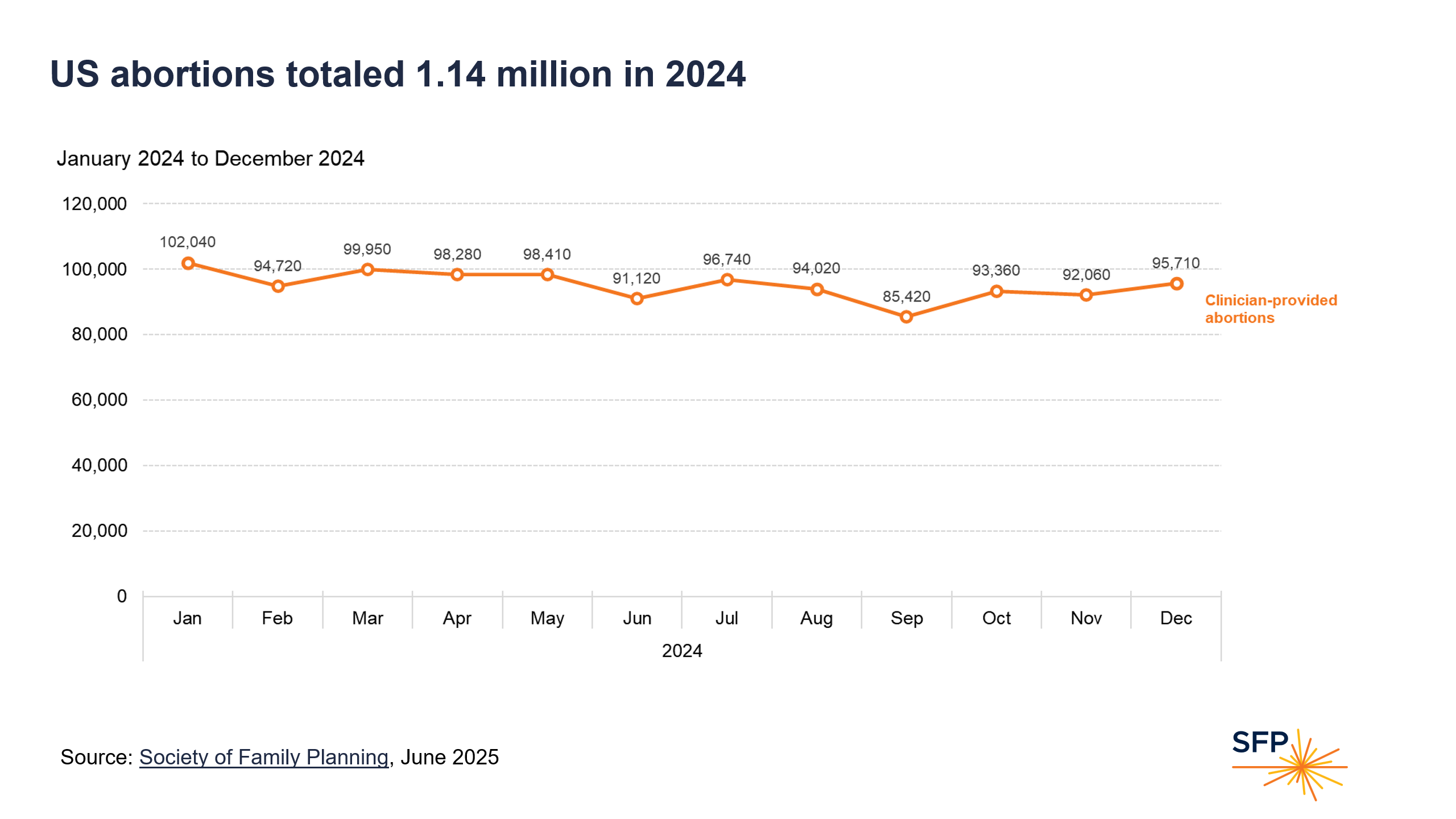
US abortions totaled 1.14 million in 2024
In 2024, 1.14 million abortions occurred in the US, the largest number of abortions in the US in recent years. The monthly total peaked in January 2024, reaching over 102,000 abortions in a single month.
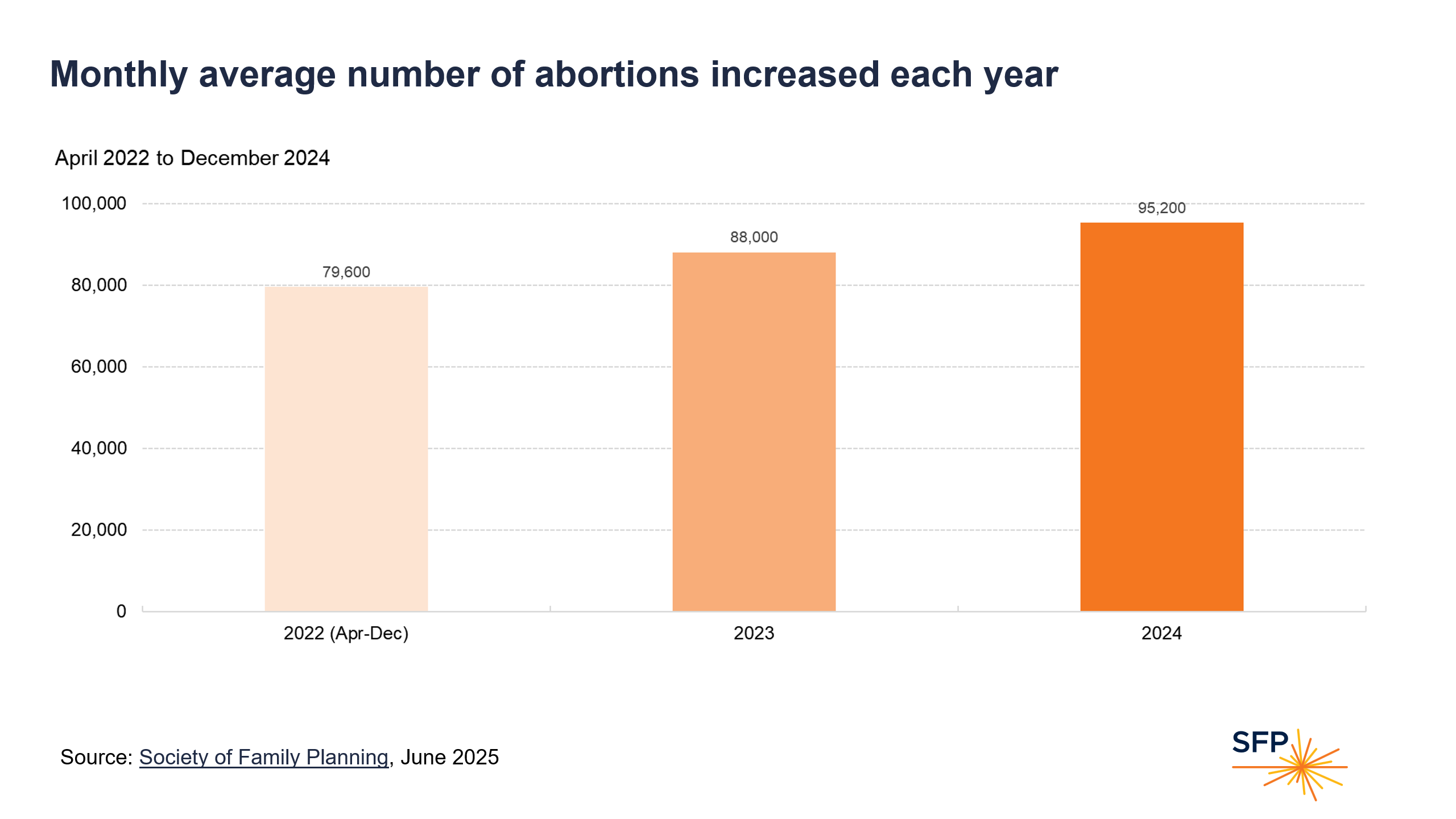
Monthly average number of abortions increased each year
The monthly average number of abortions climbed from around 80,000 in 2022, to 88,000 in 2023, to 95,000 in 2024.
Note that the 2022 monthly average is less precise because it reflects only April to December of that year; we did not collect data in January to March, which, in subsequent years, had higher volume of abortions. In addition, these months were pre-Dobbs, before abortion bans were enacted.
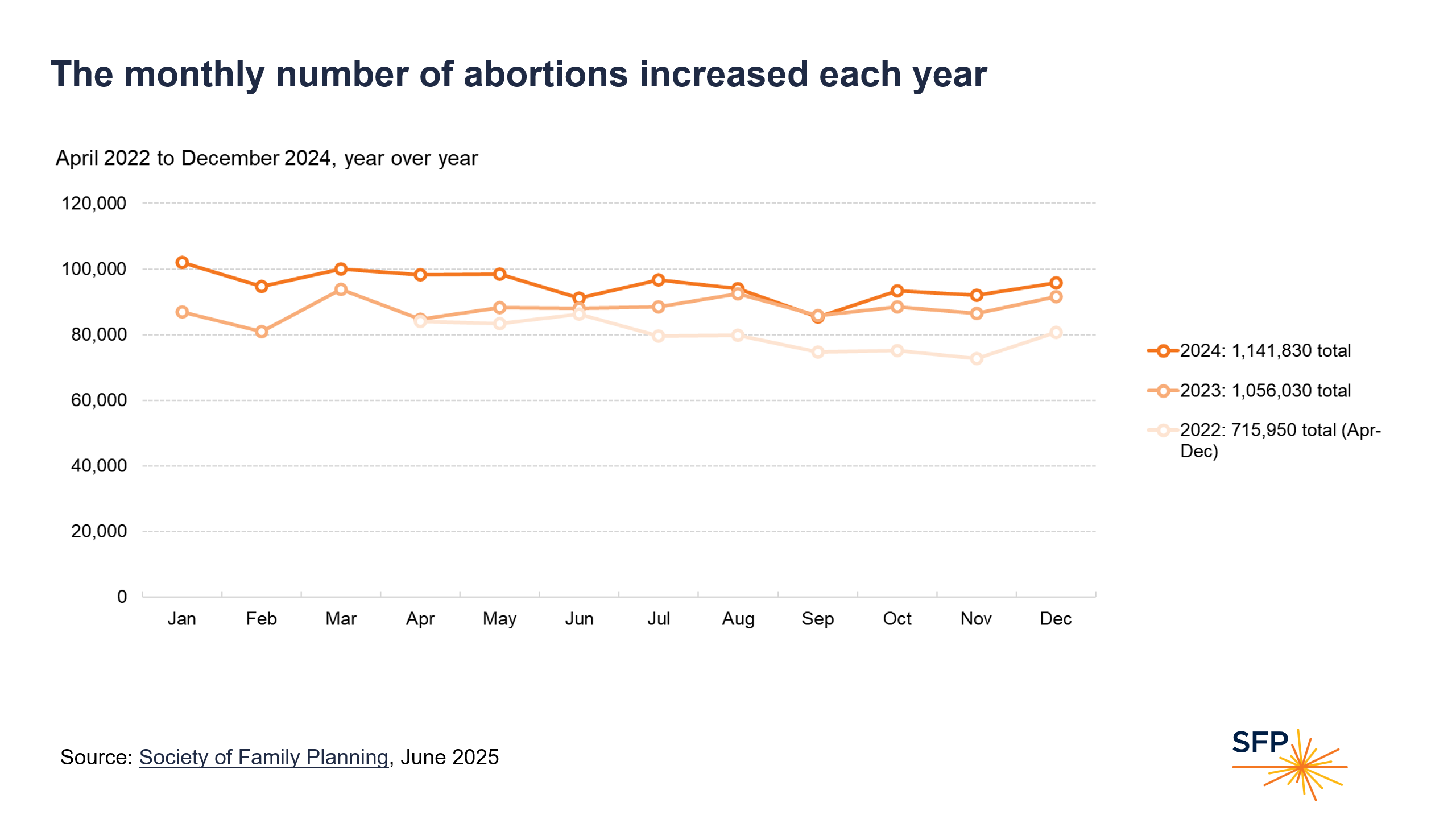
The monthly number of abortions increased each year
Comparisons of year over year show that for most months the number of abortions in 2024 was higher than the number of abortions in the same month of 2023 or 2022.
Telehealth findings
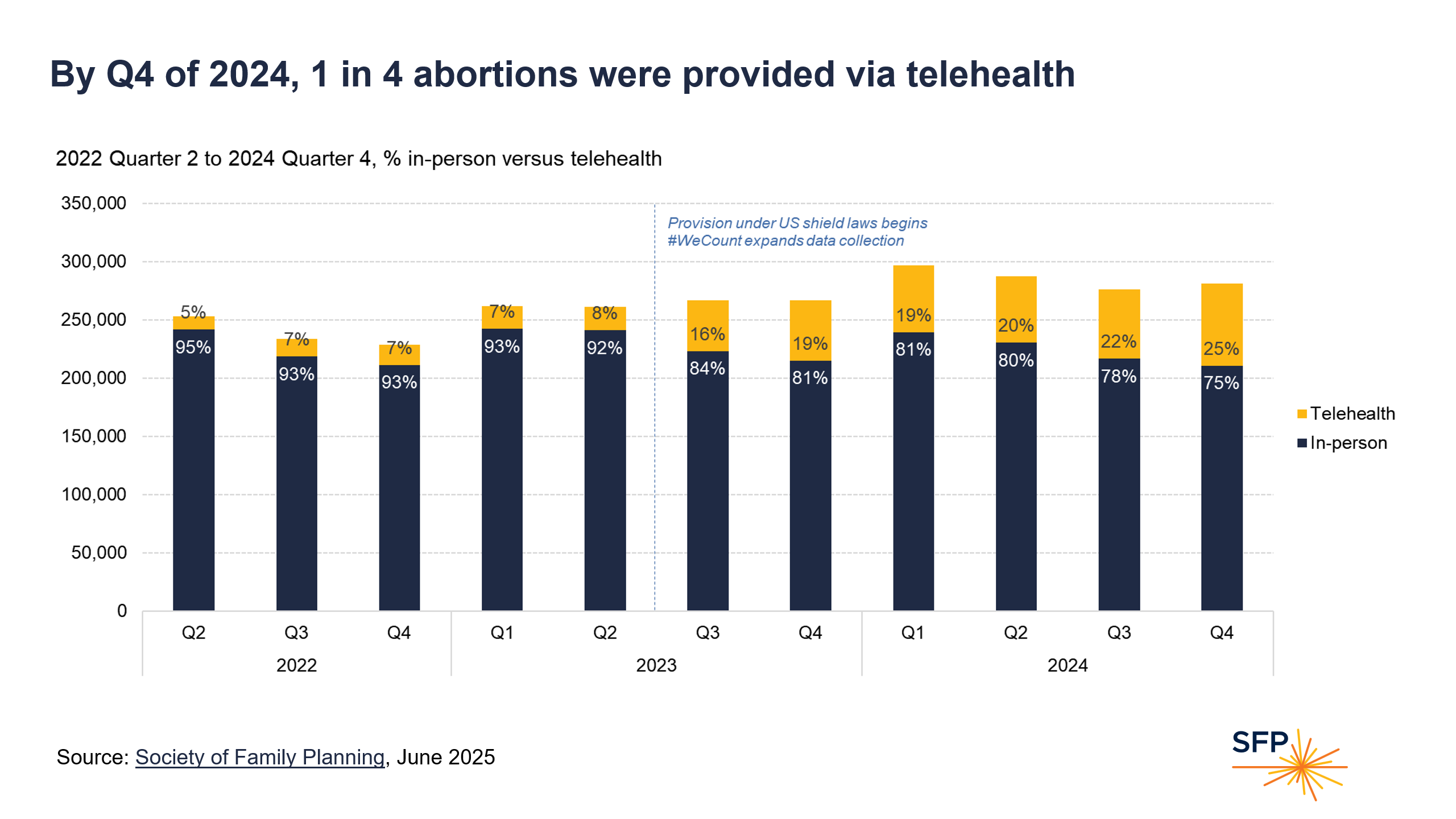
By Q4 of 2024, 1 in 4 abortions were provided via telehealth
The proportion of abortions that were provided via telehealth increased over time from 5% in April-June of 2022 to 25% by the end of December 2024.
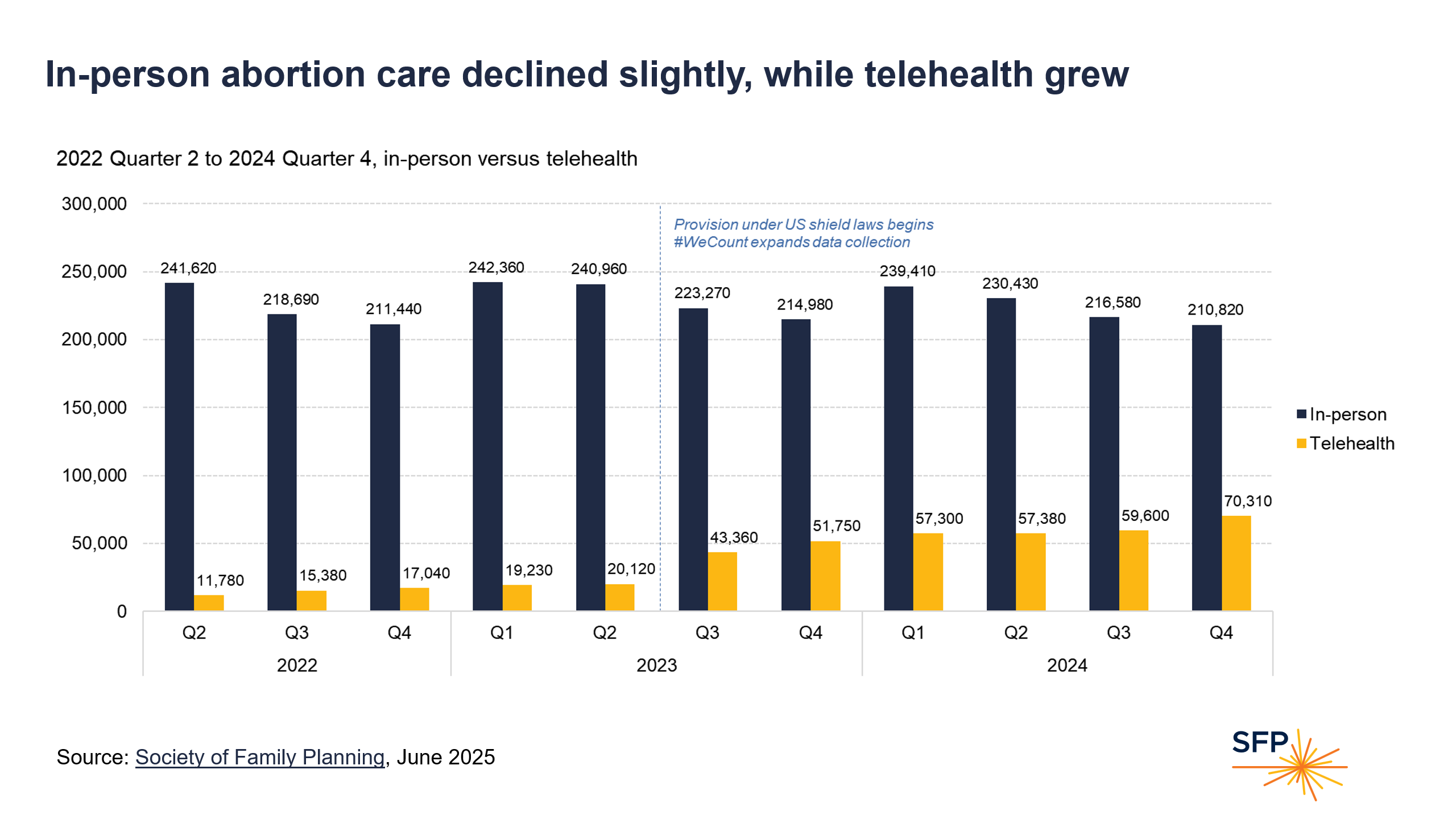
In-person abortion care declined slightly, while telehealth grew
Telehealth abortion care (which involves mailing medication abortion pills) increased both in proportion and in absolute numbers over the study period. In-person abortion care (which includes both procedural abortions and medication abortion pills dispensed in person), was much more common than telehealth abortions. As telehealth has grown, the number of in-person abortions has not declined commensurately. The number of in-person abortions was lower in the second half of each year compared to the first half.
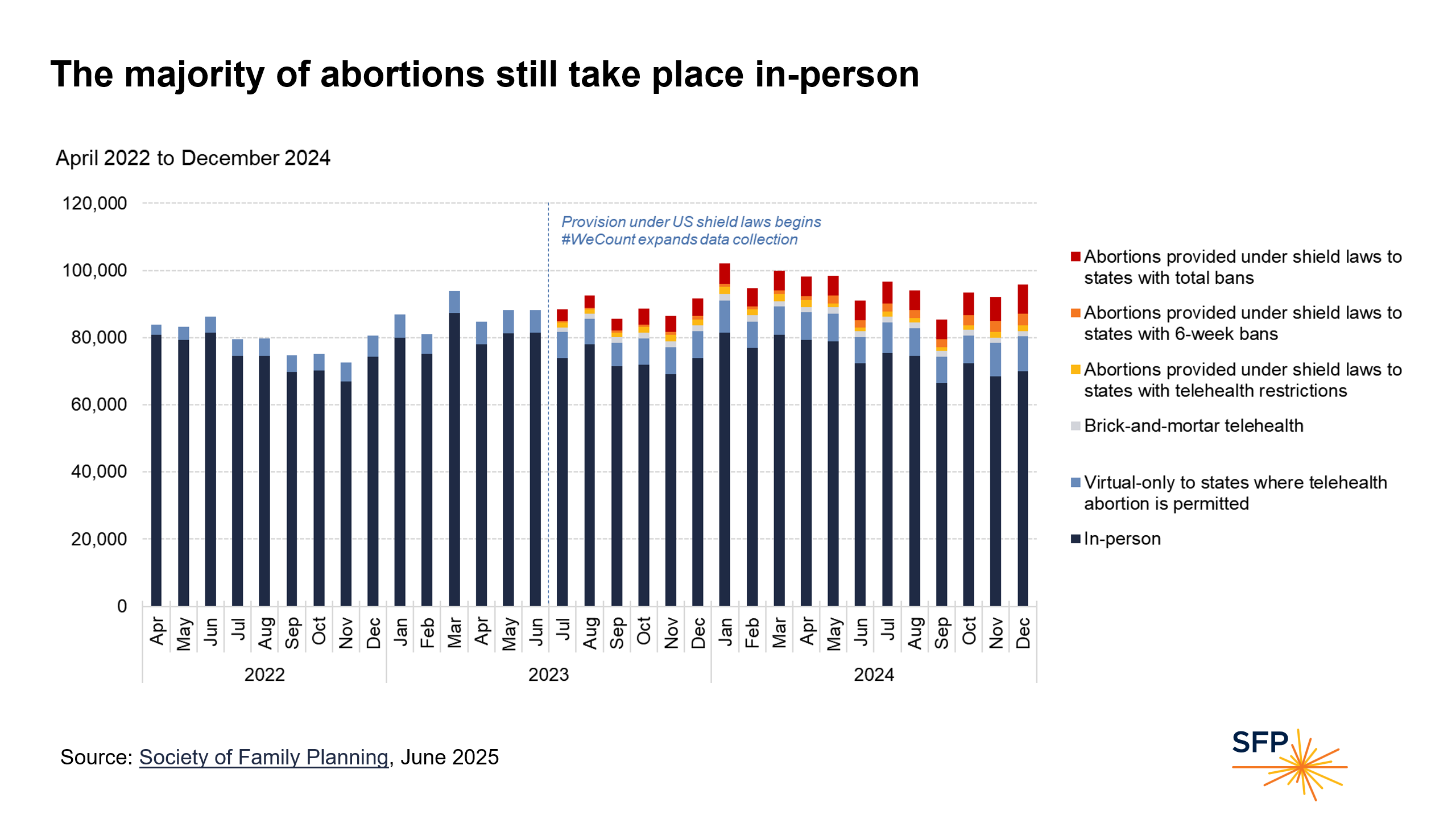
The majority of abortions still take place in-person
In the US, in-person provision continues to represent the majority of abortion care.
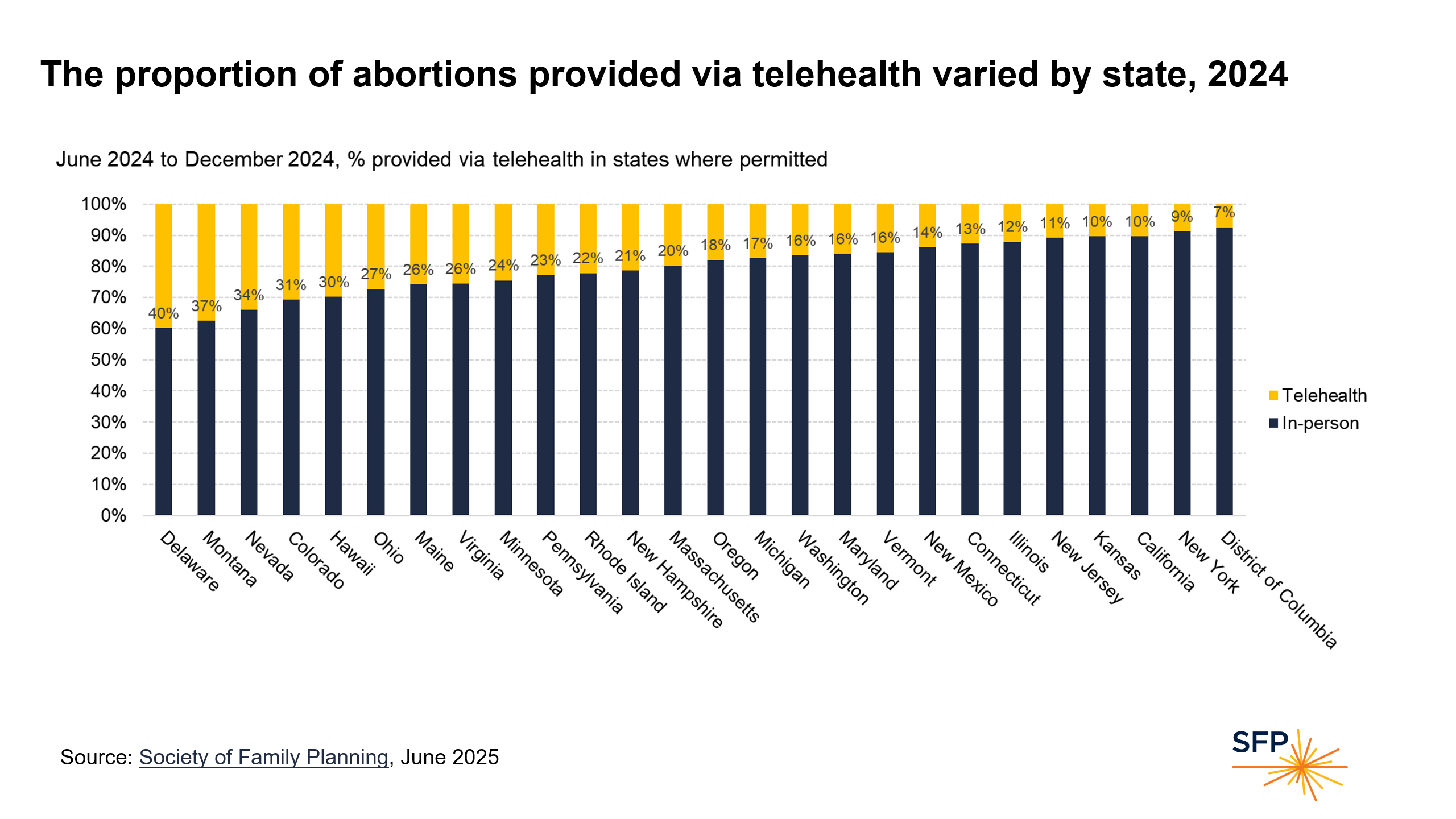
The proportion of abortions provided via telehealth varied by state, 2024
Across the US, in states that permit abortion and telehealth provision of abortion, there is substantial variation in the proportion of abortions provided via telehealth, ranging from 7% to 40%. In several larger states, telehealth is a smaller share of the abortions, at about 9-12% of all abortions.
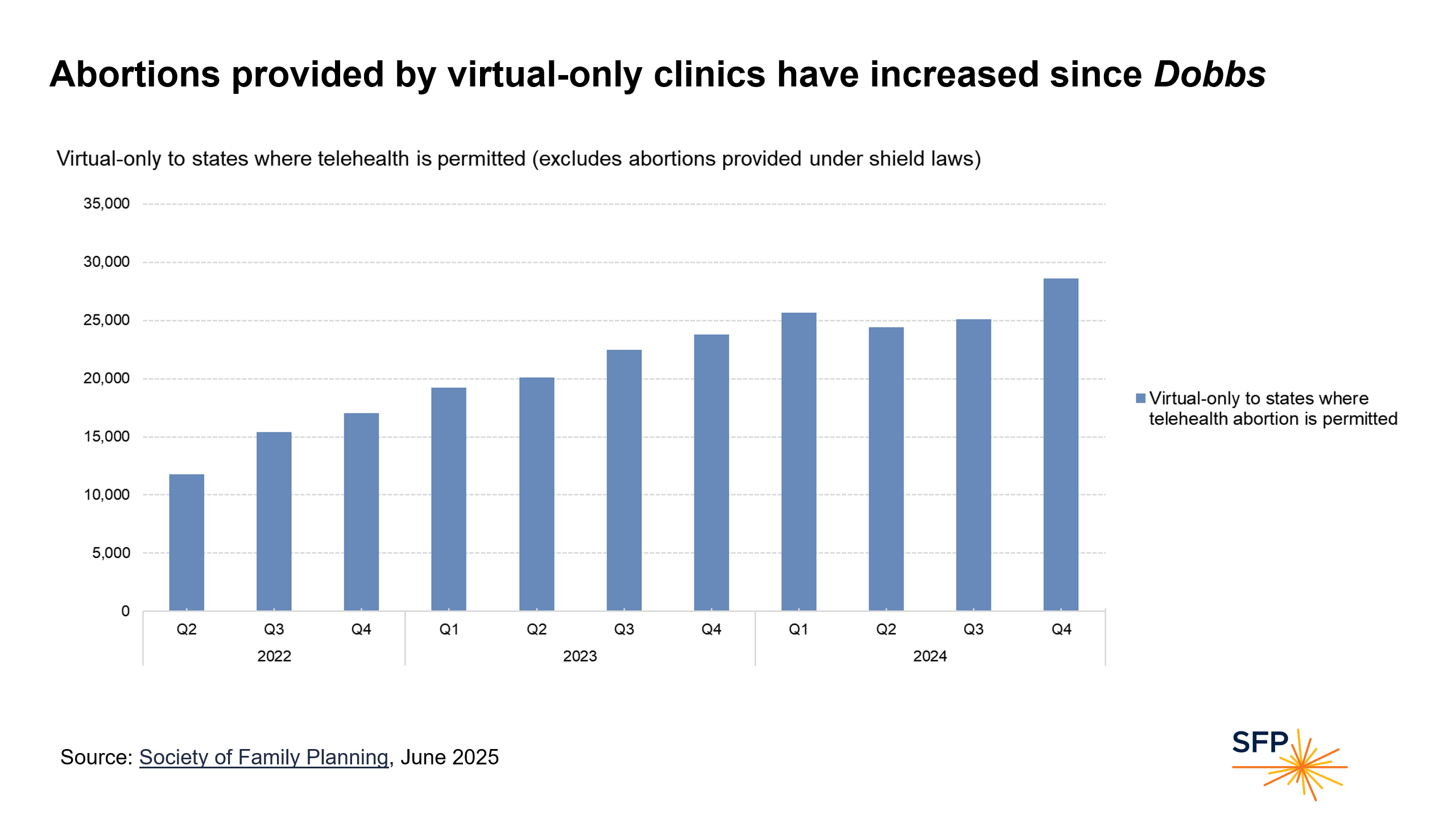
Abortions provided by virtual-only clinics have increased since Dobbs
Virtual clinics (those that that are online only and have no brick-and mortar clinic) in states that permit abortion and telehealth abortion have provided an increasing number of abortions since 2022.
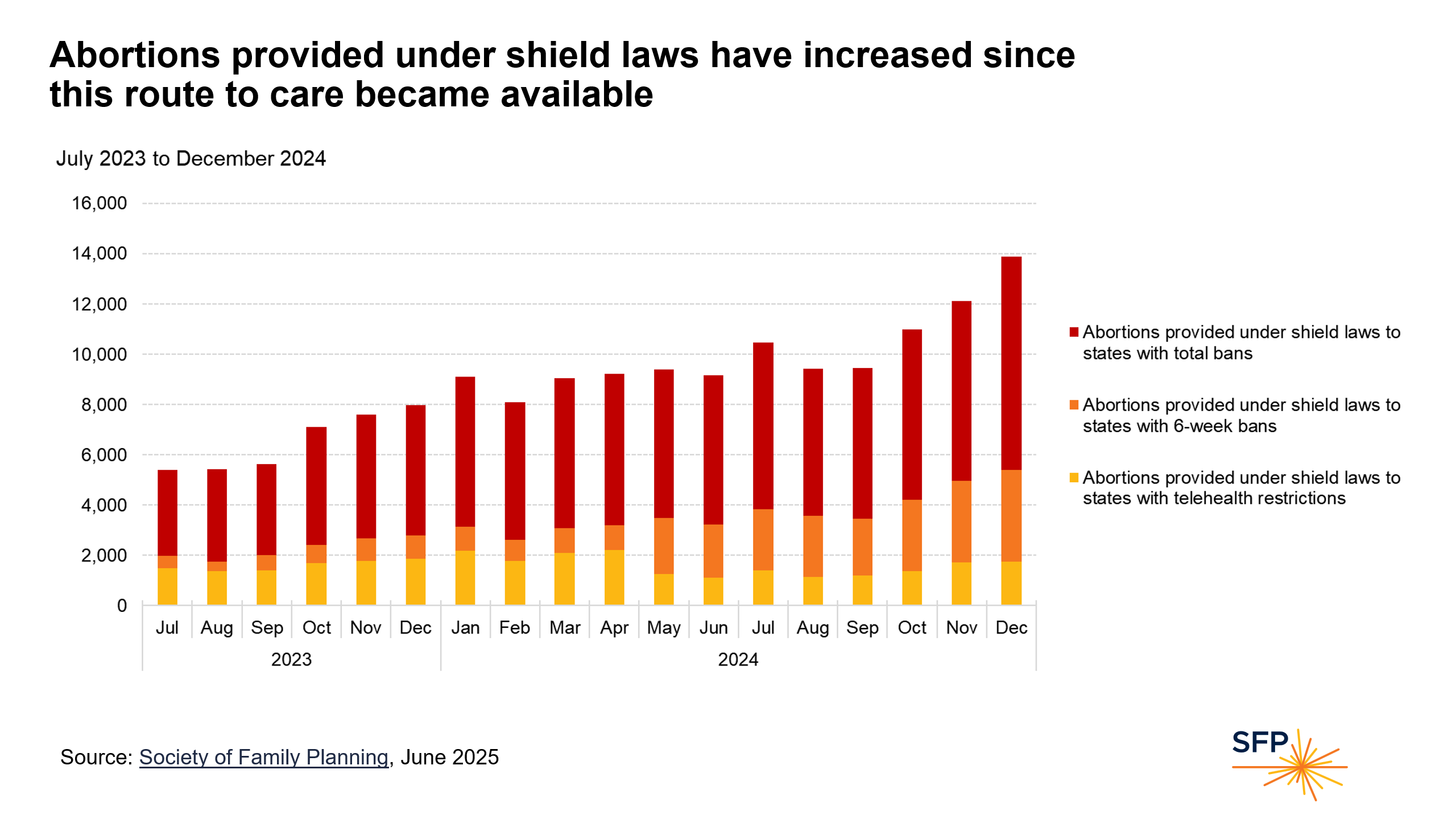
Abortions provided under shield laws have increased since this route to care became available
Providing abortions under shield laws involves mailing medication abortion pills to people in states with telehealth restrictions, 6-week bans, or total abortion bans. The number of abortions provided under shield laws has increased since providers began to offer abortion under shield laws in July 2023, with notable increases in provision to states with 6-week bans and total abortion bans. Some of the increase into states with 6-week bans is due to the states switching categories, when the states transitioned from having telehealth restrictions to having 6-week bans during this time period. By December 2024, abortions provided under shield laws totaled nearly 14,000 that month.
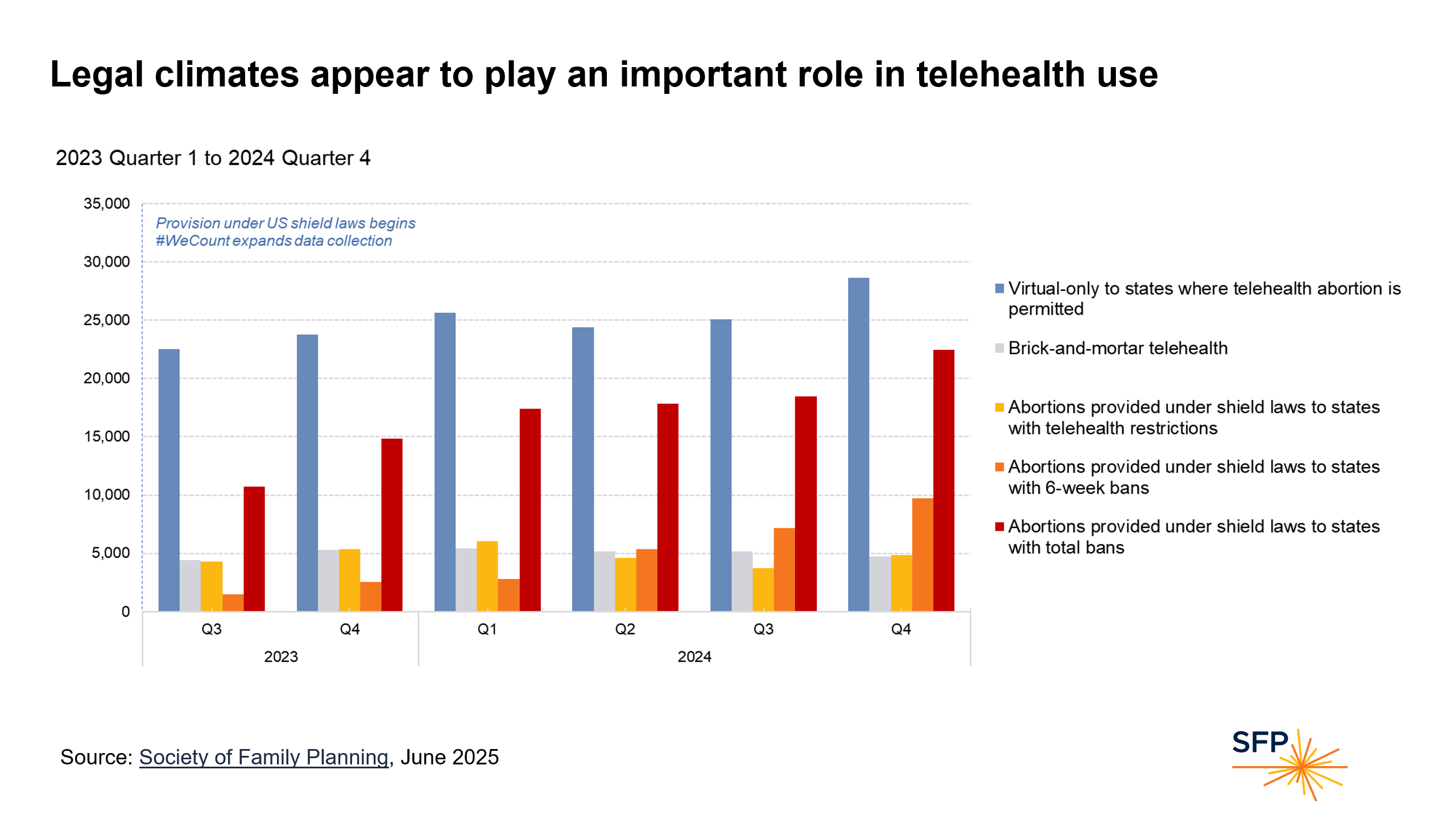
Legal climates appear to play an important role in telehealth use
Telehealth abortions provided by virtual clinics (those that that are online only and have no brick-and mortar clinic) to states that permit abortion and telehealth abortion have increased since 2023. Telehealth abortions provided by brick-and-mortar clinics have remained steady. Telehealth abortions provided into states with telehealth restrictions also remained relatively steady. Telehealth abortions provided into states with 6-week bans have increased; some of the increase into states with 6-week bans was due to the states switching from having telehealth restrictions to having 6-week bans during this time period. Telehealth abortions provided into states with total bans increased substantially by the end of 2024.
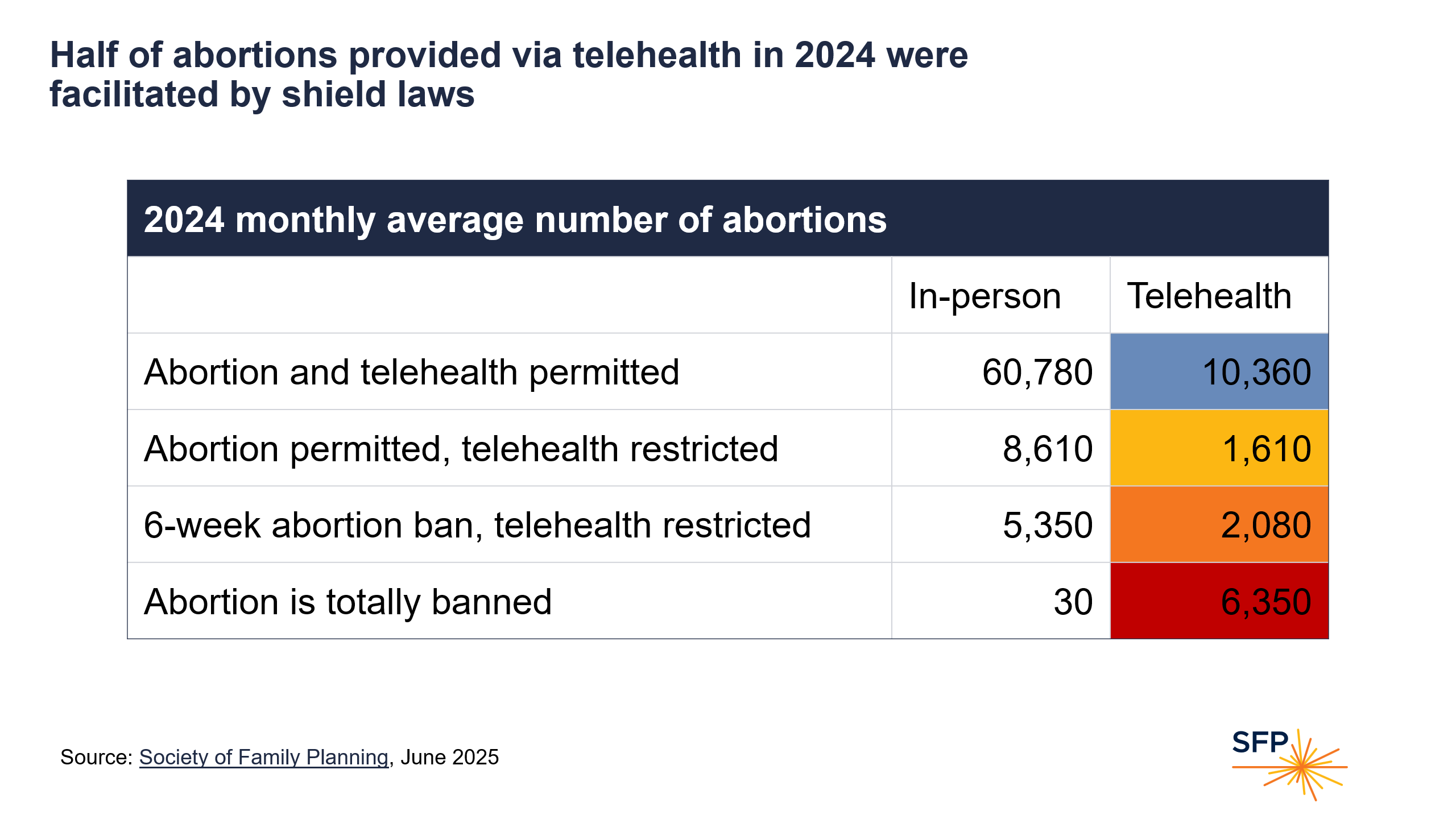
Half of abortions provided via telehealth in 2024 were facilitated by shield laws
Disaggregating in-person and telehealth and summing up across states by legal climate in 2024, there were stark differences in mode of provision, with a larger proportion of abortions provided by telehealth with each restrictiveness category. In states where abortion and telehealth were permitted, on average, 15% of abortions were provided via telehealth each month. In states where abortion was permitted but telehealth was restricted, on average 16% of abortions were provided via telehealth each month. In states with 6-week bans, on average 28% of abortions were provided via telehealth each month. In states where abortion was totally banned, there was a monthly average of only 30 abortions provided in-person, under so-called exceptions, and over 99% of abortions were provided by telehealth. In 2024, the monthly average number of abortions provided under shield laws was about 10,000 per month. Abortions provided under shield laws accounted for 49% of all abortion provided via telehealth in 2024.
Background
#WeCount is a national effort that aims to report the monthly number of abortions in the US, by state and month starting in April 2022. #WeCount data include clinician-provided abortions, defined in this report as medication or procedural abortions completed by a licensed clinician within the US in a clinic, private medical office, hospital, or virtual-only clinic. This report does not reflect any self-managed abortions, defined as ending a pregnancy outside the formal healthcare system. These data reflect the status of abortion provision in the US and can be used by healthcare systems, public health practitioners, and policymakers so that their decisions can be informed by evidence.
Terminology
Delivery settings
- Brick and mortar clinic: A physical clinic where a patient can go to receive care
- Virtual-only clinic: An online-only provider
Delivery methods
- Brick-and-mortar telehealth: Telehealth abortions offered by a brick-and-mortar clinic
- In-person care: Abortions in which a clinician meets with the patient face-to-face; can be procedural or medication abortions
- Self-managed abortion: Abortion using medications, herbs, or something else, or obtaining pills from friends or online without clinician assistance
- Telehealth abortion: Medication abortion offered by a clinician through remote consultation with the patient, resulting in remote dispensing of medications by mail
Types of care
- Medication abortion: Abortion performed with medications, including mifepristone, misoprostol, and misoprostol alone
- Procedural abortion: Abortion performed with instrumentation, including uterine aspiration (manual or electric), dilation and curettage, dilation and evacuation, or dilation and extraction
Legal context
- Shield laws: Legal protections put in place by some states to reduce legal risk for clinicians who offer abortions to patients in states where abortion is prohibited or severely restricted
Methods
In early 2022, #WeCount developed a database of all clinics, private medical offices, hospitals, and virtual clinic providers in the US known to offer abortion care. We started with the Abortion Facility Database from Advancing New Standards in Reproductive Health (ANSIRH) at University of California, San Francisco. Throughout the study period, we added new providers to our database as we became aware of them, using AbortionFinder.org and INeedanA.com to conduct regular searches in all 50 states and the District of Columbia. This report also includes abortions provided under shield laws by US-based licensed providers who are following their own state law. The Society provided compensation to participating facilities for each monthly submission.
The data in this report includes the monthly counts reported by providers for April 2022 through December 2024. In total, 83% of the abortions across the study period were based on data obtained from providers or health departments, while the remaining 17% of the data were imputed. The magnitude of imputation in each state is noted with symbols in the data tables. In 18 states, all known providers reported to #WeCount; we imputed any months not reported by these providers. For these imputations, we calculated the average percent change in abortion volume in the state and imputed values for providers with missing months. In the remaining 33 states and Washington, DC, some providers never reported to #WeCount; for these providers we imputed all months of data. To develop our imputations, we used information from news articles, contacts known to the non-reporting clinics, knowledge of the abortion volumes by state, or the median #WeCount number for the clinic or hospital type. To compute medians, we categorized reporters to #WeCount into five types of facilities and calculated the median for April and May 2022 for each category: 1) small abortion clinics, 2) large abortion clinics, 3) primary care clinics, 4) low volume hospitals, and 5) high volume hospitals. In ten states we also used publicly available state administrative data to supplement our estimates. We developed separate imputations for virtual clinics that did not submit data to us, using the median number of abortions that were provided by other virtual clinics in the state.
We reported the number of abortions by state and by restrictiveness level using three categories: states that banned abortion, states that restricted abortion to before detection of embryonic cardiac activity, also referred to as a “6-week bans” because detection of such activity usually occurs around that point, and states that permitted abortion. These categories were based on the abortion policy in each state on the 15th of each month as reported by the New York Times. For a legal analysis of restrictions that prevent explicitly ban telehealth or implicitly preclude telehealth abortion, we rely on the RHITES map. Monthly state totals were rounded to the nearest 10.
#WeCount was deemed exempt by Advarra IRB. All major decisions were guided by a Research Steering Committee listed below. This research was sponsored by the Society of Family Planning.
Limitations
Counts are an underrepresentation of all abortions in the US. #WeCount has a comprehensive count of abortions provided by licensed clinicians, with more than 83% of all abortions reported and about 17% imputed. Abortions provided by individual hospitals and private practice clinicians may be underreported. These counts also do not include abortions that take place in the US outside of the formal health care system.
We do not have estimates of the proportion of people who did not take the medications sent to them. These data show telehealth abortions as the providers documented mailing them. Some people may not have taken the pills, and we do not have an estimate of that. Use of shield laws to provide abortion via telehealth into states with total or 6-week abortion bans or with telehealth abortion restrictions started in July 2023, and #WeCount began to count abortions provided under shield laws at that time. Because of this transition in abortion provision, #WeCount does not have a comparator for previous months.
#WeCount cannot estimate the unmet needs for abortion. Research has yet to accurately capture the underlying need for abortion. We don’t have any counts of the number of people who needed an abortion and didn’t get it.
#WeCount is designed to describe changes in abortion access and provision, rather than to explain why these changes are taking place.
Contributors
#WeCount is made possible by the many abortion providers who generously reported their data in support of this effort. This report was prepared by the #WeCount Co-Chairs and Society of Family Planning staff, with guidance from the Research Steering Committee, as well as many members of the Society of Family Planning community.
#WeCount Co-Chairs
- Alison Norris, MD, PhD; Ohio State University
- Ushma Upadhyay, PhD, MPH; University of California, San Francisco
#WeCount Research Steering Committee
- Abigail Aiken, MD, PhD, MPH; University of Texas at Austin
- Danielle Bessett, PhD, MA; University of Cincinnati
- Anitra Beasley, MD, MPH; Baylor College of Medicine
- Angel Foster, DPhil, MD, AM; University of Ottawa
- Jenny Higgins, PhD, MPH; University of Wisconsin
- Rachel Jones, PhD; Guttmacher Institute
- Isaac Maddow-Zimet, MS; Guttmacher Institute
- Caitlin Myers, PhD; Middlebury College
- Whitney Rice, DrPH, MPH; Emory University
- Hannah Simons, DrPH; Planned Parenthood Federation of America
- Mikaela Smith, PhD; Ohio State University
- Terri-Ann Thompson, PhD; Ibis Reproductive Health
- Kari White, PhD, MPH; Resound Research for Reproductive Health
#WeCount Society of Family Planning Staff
- Jenny O’Donnell, ScD, MS; Vice President of Research and Evaluation
- Claire Yuan, MPP; #WeCount Data Manager